
Preoperative Informed Consent
Components:
- Indications for the procedure
- Alternative treatment options
- Thorough explanation of the planned procedure
- Consequences of not proceeding with the surgery
- Benefits of surgery and how it will impact her quality of life
- Risks of the procedure
- See below
- Expected length of hospitalization or post-op plan (discharge home, etc.)
- Expected length of recovery and limits associated with recovery time
- Anticipated return to normal and activities and work
- Long term effects of the surgery, failure rates, and risk of reoperation
The biggest question most new learners have is how in depth their discussion of risks and complications of the procedure should be. A general rule for informed consent is if a complication occurs more than 1% of the time discuss it specifically in an absolute risk way (i.e. 1 in 80 will develop infection that requires antibiotics). If the complication happens in <1% of patients don’t go into specifics but instead make a general statement about the possibility. For example the risks of vaginal hysterectomy are all <1%, therefore, a consent should be general and look something like this: ” Complications of this procedure are risk of injury to surrounding structures, infection, blood loss, blood clots, and associated risks with general anesthesia like aspiration.”
Surgical Wound Classifications
Antibiotics for surgery are decided based on the type of procedure performed and its surgical wound classification as defined by the American College of Surgeons: clean, clean-contaminated, contaminated, dirty
- Clean: Clean surgical wounds show no signs of inflammation and do not involve the respiratory, gastrointestinal or genitourinary tracts. Laparoscopic surgeries, surgeries involving the skin (such as biopsies), eye or vascular surgeries are good examples.
- Clean-contaminated: Clean-contaminated wounds are clean wounds with a higher risk of infection such as those involving the gastrointestinal, respiratory or genitourinary tracts, as long as the surgery is uncomplicated. Any wound opened to remove pins or wires, chest procedures, ear surgeries, or gynecologic procedures are considered class II surgical wounds.
- Contaminated: Contaminated wounds are created when an outside object comes in contact with the wound. This could be a bullet, knife blade or other pointy object. Or the contamination could be caused by large amounts of spillage from the GI tract into the wound. Any highly inflamed or infected tissue around a surgical wound is considered contaminated.
- Dirty: Dirty-infected surgical wounds include those with a foreign object lodged in the wound (such as a bullet or other debris). This class also includes traumatic wounds from a dirty source where the treatment was delayed, infected surgical wounds or any wound that has been exposed to pus or fecal matter.
Preoperative Antibiotics for Gynecology
Administration of preoperative antibiotics should occur 1 hour prior to incision. Ancef (cefazolin) is usually the drug of choice with the exception of evacuation procedures. Patients that are allergic to penicillins CAN receive Ancef, unless they have a specific anaphylactic allergy to cephalosporin drugs as well. Prophylactic Ancef is given as 2 g unless the patient is >120 kg (264 lbs) then 3 g is recommended. If the patient has an allergy to cephalosporins the alternative antibiotic choice is either clindamycin OR metronidazole + gentamicin OR aztreonam.
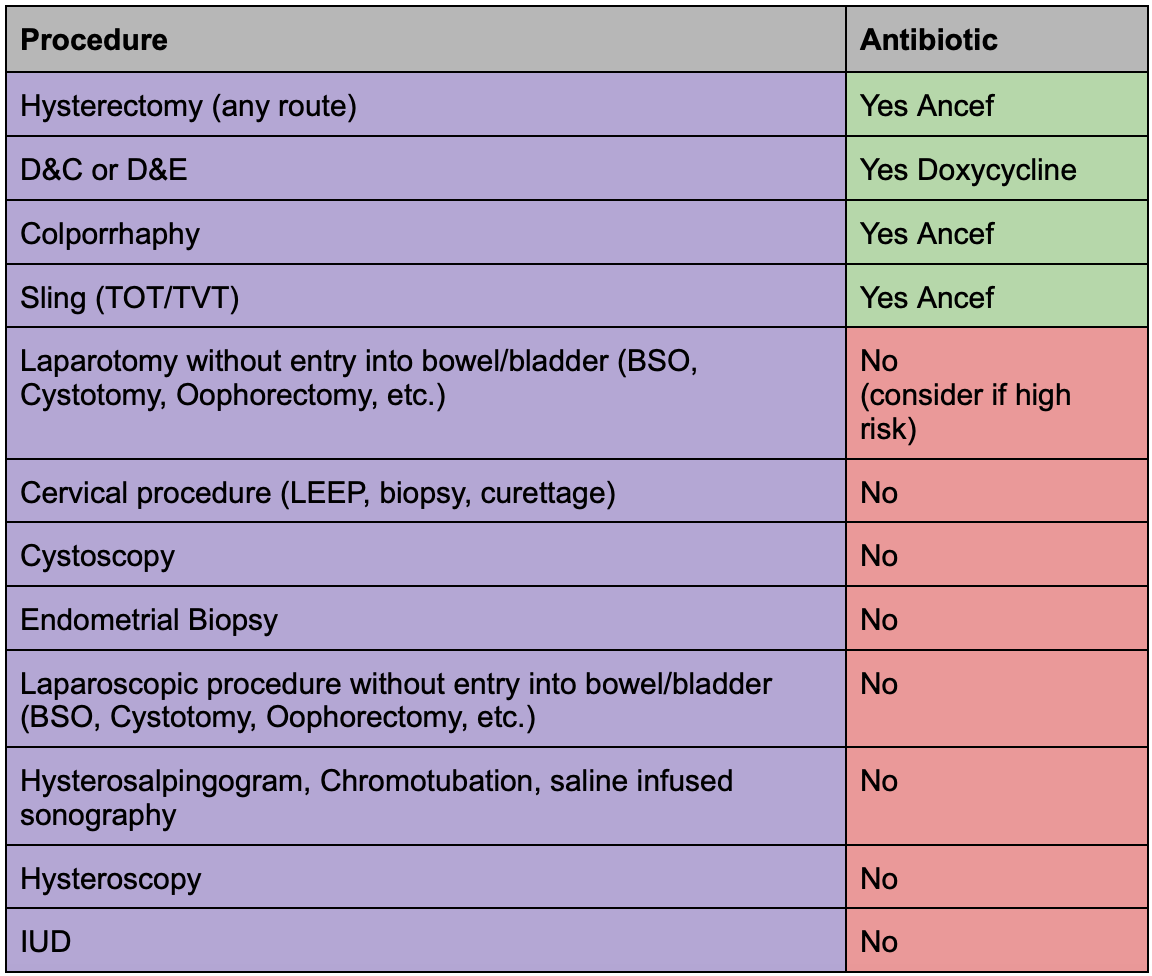
Vaginal
Any vaginal entry in surgery classifies the wound as clean-contaminated. We worry about polymicrobial aerobic and anaerobic flora from the vagina contaminating the wound. The antibiotic of choice for any vaginal entry procedure (hysterectomy, TOT/TVT, colporrhaphy) is Ancef.
Abdomen
Gynecologic procedures done laparoscopically or by laparotomy that do not have vaginal entry are considered clean procedures that do not require prophylactic antibiotics. Infection following these would be due to skin flora.
Intrauterine/Cervical
Procedures that pertain to the cervix or that enter the uterine cavity without any incision through the vagina such as a hysterosalpingogram, hysteroscopy, sonohysterography, IUD, or endometrial biopsy are considered clean-contaminated however the risk of infection is low and they do not require any prophylactic antibiotic use. The only time an antibiotic, doxycycline, should be considered is if there is a history of PID in someone undergoing hysterosalpingogram.
Thromboprophylaxis for Gynecology
Determine the Caprini Score
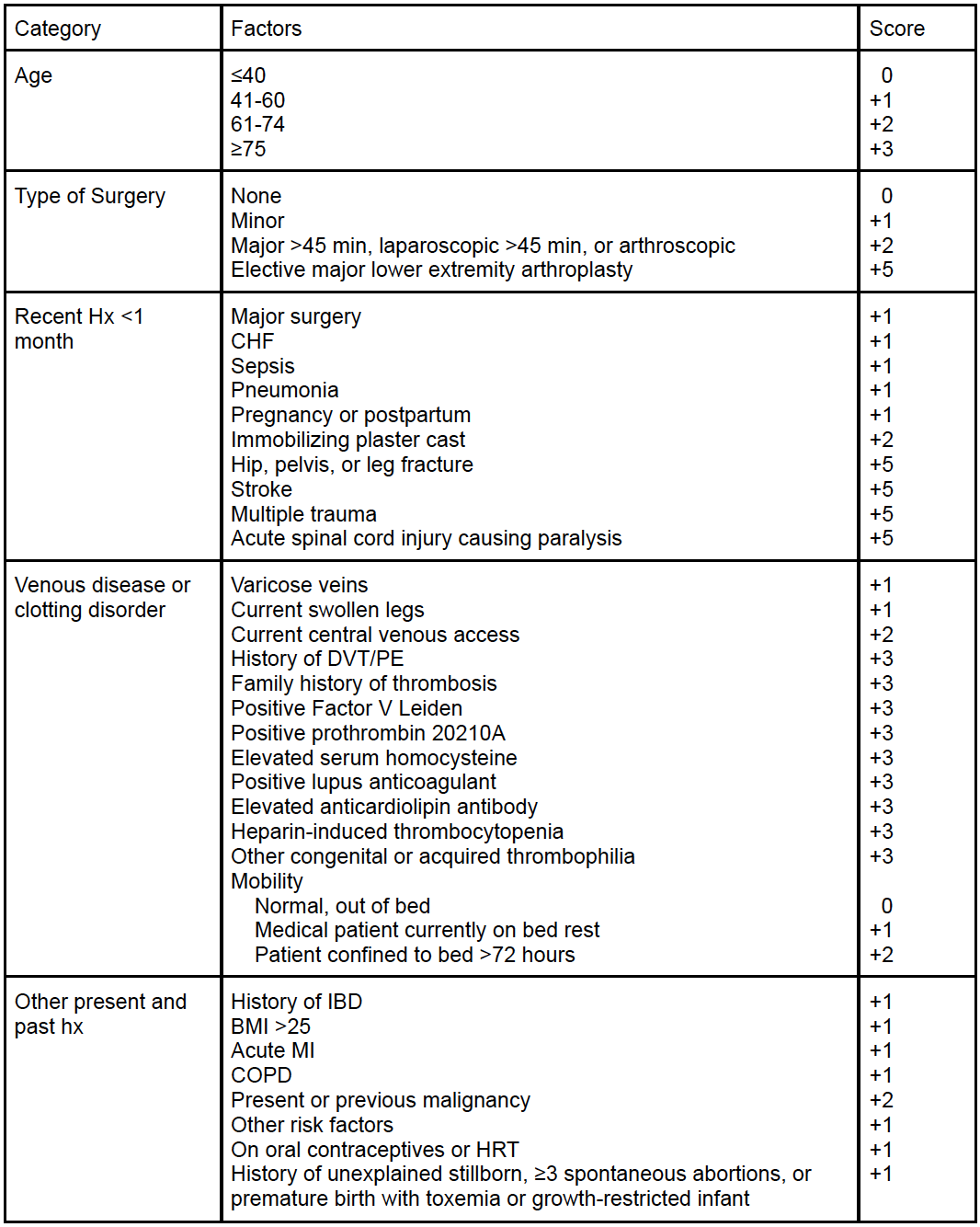
Recommended Prophylaxis Based on Score:
| Caprini Score | Risk category | Risk % | Recommended prophylaxis** | Duration of chemoprophylaxis |
| 0 | Lowest | Minimal | Early frequent ambulation only, OR at discretion of surgical team: Pneumatic compression devices OR graduated compression stockings | During hospitalization |
| 1–2 | Low | Minimal | Pneumatic compression devices ± graduated compression stockings | During hospitalization |
| 3–4 | Moderate | 0.7% | Pneumatic compression devices ± graduated compression stockings | During hospitalization |
| 5–6 | High | 1.8% | Pneumatic compression devices AND low dose heparin OR low molecular weight heparin | 7–10 days total |
| 7-8 | High | 4.0% | Pneumatic compression devices AND low dose heparin OR low molecular weight heparin | 7–10 days total |
| ≥9 | Highest | 10.7% | Pneumatic compression devices AND low dose heparin OR low molecular weight heparin | 30 days total |
Preoperative Antibiotics for Obstetrics
- Ancef is the prophylaxis of choice for cesarean section. The only time it is not used is in the setting of chorioamnionitis where the patient is already on antibiotics with appropriate coverage (ampicillin + gentamicin +/- clindamycin if endometritis suspected).
- Azithromycin infused over 1 hr. is recommended in addition to Ancef for nonelective cesarean deliveries (aka deliveries where mother has been laboring with a broken water and an emergent or unplanned cesarean occurs)
Thromboprophylaxis for Obstetrics
(SMFM recommendations)
- All women should receive pneumatic compression devices preoperatively until they are ambulatory postoperatively (Grade 1C- strong recommendation, low-quality evidence).
- Suggestions by SMFM with Grade 2C evidence (weak recommendation, low-quality evidence):
- Hx of prior DVT or PE they should receive sequential compression devices + LMWH preop and continued 6 weeks postop (40mg subcutaneous daily unless obesity >40 BMI then q12)
- Personal hx of an inherited thrombophilia but no previous thrombosis it is recommended to do both sequential compression devices + LMWH preop and continued 6 weeks postop.
It is important to note that while these are recommendations, they do not have strong supporting evidence. Most hospitals have policies that you will abide by. Understand that policies and evidence-based practice can be two very different things.
Postoperative Considerations and Surgical Complications
Wound Care
This wound care manual put out by the American College of Surgeons is meant for patients, however, it is a good read for students so that they are able to discuss wound care with patients, answer questions, and help staff by understanding the basics of wound care and dressing patients before discharge, depending on the wound type.
Surgical Patient Education Program: Surgical Wound Care
